LETTER | It is quite clear that we need to use the Covid-19 vaccine to overcome the coronavirus pandemic. If a significant portion of our population were to be immune – even partially or for a period of one or two years – then the rate of transmission of the coronavirus would drop.
That would mean we can reduce the level of physical distancing, and more people can return to their jobs and businesses, and our economy can begin recovering.
Close to 60 Covid-19 vaccines are being developed, and a few are already being administered on a mass basis. But it is important to do it right and to make sure that the "cure" doesn’t cause new health problems.
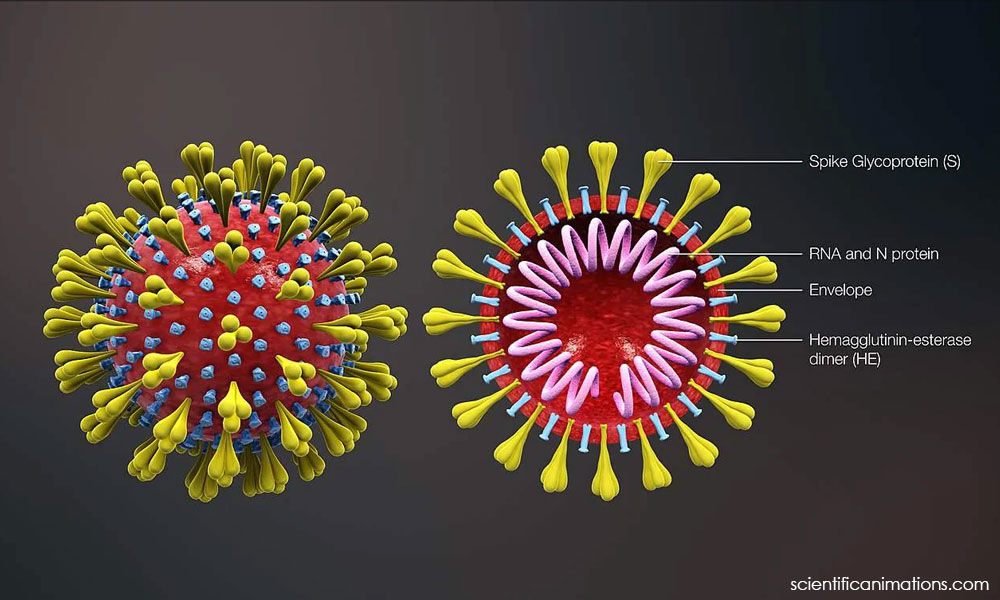
Vaccines work by presenting a viral protein or proteins to the subject to coach the subject’s immune system to develop antibodies that can neutralise the real virus if and when the real virus attacks the subject.
We can divide the Covid-19 vaccines into two main groups:
- Vaccines that use inactivated viruses or laboratory-manufactured Covid-19 protein to stimulate this immune response
- Vaccines that use a new technology that makes the subject’s own body produce the Covid-19 protein that then stimulates the subject’s immune system to produce the neutralising antibodies
‘Old-tech’ vaccines
The first group of vaccines rely on old and tested technology that we have been using for the past 50 years for various diseases. The medical community is familiar with the potential downsides of this first group. These include insufficient inactivation of the virus, which means the virus is still able to replicate in the subject’s body.
Side effects may occur due to the chemicals used to inactivate the virus or due to the various adjuvants used to enhance the body’s reaction to the viral protein. (Aluminum is one of the adjuvants used to “irritate” the immune system.)
More sophisticated vaccines
The second group of Covid-19 vaccines comprises RNA or DNA which instructs our cells to make the Covid-spike protein when this genetic material is injected. This approach is new and has not been used in the production of any vaccines for a mass vaccination campaign.
This canggih approach involves injecting the genetic code for the Covid-19 spike protein into the subject’s body. This genetic code enters the subject’s cells and tricks the subject’s ribosomes to produce thousands of copies of the spike protein.
Ribosomes are the organelles within our cells that produce proteins, as instructed by the nucleus of the cell. The nucleus sends out messenger RNA to the ribosomes to tell it what type of protein to produce.
These modernistic vaccines rely on messenger RNA that codes for the Covid-19 protein.
In the Pfizer and Moderna vaccines, the messenger RNA (mRNA) that codes for the Covid-19 spike protein are put in minute phospholipid capsules, and many of these capsules are injected into the subject.
These capsules circulate in the blood and slip into certain cells in the body where the mRNA instructs the ribosomes of these cells to manufacture the Covid-19 spike protein.
Some of these spike protein molecules extrude from the cells into the bloodstream and catch the attention of the immune system, which then produces antibodies against these spike proteins. The spike proteins sticking out of the “infected” cells also induce killer lymphocytes to attack and kill these cells.
It is possible that these modern vaccines are more effective than the traditional ones in that they induce more cell mediated-response (the killer lymphocytes).
But that is part of the problem with them. These modern vaccines involve the destruction of some of the subject’s cells. Do the developers of these vaccines know for sure that their phospholipid capsules will not slip into nerve cells or into kidney cells? These tissues are not particularly capable of regenerating themselves if they are damaged.
We also do not know the longer-term consequences of exciting the body’s immune system and then exposing that system to cellular antigens released by the destruction of the RNA ‘infected’ cells. Might this induce an auto-immune disease in a portion of the people so exposed?
Auto-immune diseases are conditions in which the body’s immune system starts attacking some component of the body. Rheumatoid arthritis is one example of auto-immune disease and we still do not understand why it affects certain people or what sets it off.
Would Covid-19 vaccines that rely on generating viral proteins within our own cells precipitate auto-immune disease in those so predisposed? We do not know. It may not happen, but shouldn’t we make sure that it doesn’t before we inject this vaccine into millions of people?
The Oxford-AstraZeneca and Sputnik V vaccines use a different strategy to deliver the Covid-19 genetic code for the spike protein to the subject's cells.
They convert the Covid-19 code into DNA, which is more stable and does not require ultra-cold storage. They then put this DNA into modified Adenoviruses which are incapable of replicating in the subject’s body. These modified Adenoviruses deliver the DNA code to the subject’s cells.
As Adenoviruses cause respiratory tract infections, these vaccines will infect respiratory tissues and are less likely to affect nerve and kidney cells.
But as these vaccines use DNA to code for the spike protein, the vaccine-delivered DNA has to go into the nucleus of the subject’s cell to produce the messenger RNA that can instruct the subject’s ribosomes to produce the spike protein.
Willfully putting foreign DNA into the nucleus of human cells is something we should not take lightly. We know that in certain viral infections, viral DNA becomes incorporated into human chromosomes. This occurs in hepatitis B and HIV infections.
Do we know for sure that this will not occur, in perhaps a small percentage of cases, with the Covid-19 vaccines that use DNA? Will this viral gene interact with any other gene in our genome and cause a health problem? Maybe not, but should we take that risk?
Look at the alternatives. Let us be clear here. I am not an "anti-vaxxer". Vaccines have played a huge role in the control of infectious diseases in the past 50 years, and they certainly have a big role to play in the future.
The crucial question is, do we need desperate measures such as deploying the new RNA and DNA vaccines on a global scale before checking carefully that they do not cause unexpected negative effects in the medium to long-term?

After all, there are other effective alternatives. Several vaccines have been produced using traditional technology. These ‘old-tech’ vaccines do not rely on RNA or DNA and do not involve the subject’s cells in the generation of the viral antigen.
The old-tech vaccines comprise Covid-19 virus proteins that can be injected into the subject’s body. These include CoronaVac, the Zhifei vaccine, and Novavax. There are several more.
Why not use these old-tech vaccines to control the pandemic? Why go for modern technology that hasn’t been properly assessed and might have serious side-effects in the medium to long-term?
Don’t be naive
The insistence of many vaccine manufacturers on indemnity clauses in the agreements with governments is clear evidence that the manufacturers themselves are also not able to exclude serious medium or long-term side effects.
We would be extremely naive if we do not note the profit motive when evaluating our national vaccine strategy. Vaccine manufacturers stand to make humongous profits if their vaccines are used on a worldwide scale. With the indemnity clause in place, they are shielded from litigation if anything goes wrong.

We have to be world-wise and factor in the tremendous influence that the large pharmaceutical companies have over governments and regulatory institutions in the West.
We also have to factor in geopolitical biases when evaluating Western media often disparaging news reports of non-Western vaccines.
A cautious approach
Malaysia is not in as dire straits as the US or the EU countries where the failure to implement physical distancing measures has led to the current horrendous levels of infections and hospitalisations.
My friends and I would like to suggest the following:
- Rely on "old tech" vaccines that inject viral protein into the subject. Let’s not experiment on our population with the canggih vaccines that use the new RNA and DNA technology, whose medium and long-term adverse effects are at present unknown.
- Offer the "old tech" Covid vaccines to the high-risk groups initially – e.g. healthcare workers, other frontline personnel, older people, people with comorbidities (other health problems) – and then later to the entire population. But do not make it mandatory for any particular group. Let people make an informed choice.
- Provide clear information to the public. All vaccines have side effects and the public has a right to know of these. Given the level of mistrust of authorities in the West, some of the doubts expressed there will filter over to Malaysia. The best way of dealing with this mistrust is by being honest with our people. The authorities should tell the people what they know, and also what we still do not know about these vaccines.
- Provide the "old tech" Covid-19 vaccines free to the population.
- Conduct post-Covid-19 vaccination surveillance to obtain an accurate estimate of symptoms and side effects arising from the vaccine.
- Communicate these findings to the people so they can make an informed choice regarding getting vaccinated.
The Health Ministry is in the midst of conducting an opinion poll to ascertain the Malaysian population’s stance regarding the Covid-19 vaccine.
This is the opportunity for civil society groups and concerned individuals to voice out and call for a cautious and measured approach to the mass vaccination of the Malaysian population.
DR MICHAEL JEYAKUMAR DEVARAJ is the chairperson of Parti Sosialis Malaysia (PSM) was a two-term MP for Sungai Siput.
The views expressed here are those of the author/contributor and do not necessarily represent the views of Malaysiakini.